
Niger J Paed 2014; 41 (4): 331 - 336
ORIGINAL
Ahmed PA
Clinical presentation of
Ulonnam CC
tuberculosis in adolescents as
seen at National Hospital Abuja,
Nigeria
DOI:http://dx.doi.org/10.4314/njp.v41i4,8
Accepted: 3rd May 2014
Abstract
Background: Adoles-
clinical symptoms while 2(5.6%)
cents with tuberculosis (TB) form
were
asymptomatic;
identified
Ahmed
PA
a
significant proportion of child-
during contact tracing as latent TB
Ulonnam CC
(
)
hood
TB cases presenting with
infection (LTBI). Abnormal chest
Department of Paediatrics,
specifics clinical patterns.
radiograph findings were; wide-
National Hospital,
Objective: To
describe the
clinical
spread lung infiltrate in 10(27.8%),
Abuja Nigeria.
hilar opacities 7(19.4%), cavita-
Email: ahmedpatience@yahoo.com
presentation of tuberculosis in
adolescent at National Hospital
tory lesions 4(11.1%), pleural
Abuja (NHA), Nigeria.
Effusion 3(8.3%) and military
Subjects and method: This
is a
opacities 1(2.7%). AFB was
descriptive
and
retrospective
isolated in 5(13.9%), while
study of adolescents aged 10- 15
23(63.9%) had a raised ESR above
years seen at the department of
30mm/hr. Twenty seven (75.0%)
Paediatrics NHA Nigeria from
of
the adolescents completed treat-
August 2009 to July 2013.
ment for tuberculosis, 7(19.4%)
Result: Thirty-
six adolescents
were lost to follow up and
diagnosed with tuberculosis were
2(5.6%) died while 4(11.1%) had
reviewed.
Adolescent
TB
ac-
re-treatment for TB from relapse.
counted for 18.8%(36/192) of
Clinical presentations were pulmo-
total cases of children aged 0-
nary TB (PTB) 22(61.1%), and
15years seen at the Department of
extrapulmonary TB
12(33.3%);
Paediatrics
Respiratory
Clinic
distributed as TB adenitis
during the study period. The mean
4(11.1%), TBM 3(8.3%), Pericar-
(SD) age was 12.3(1.76) years.
dial TB 3(8.3%), Miliary TB
Twenty seven patients (75.0%)
1(2.8%) and Spinal TB 1(2.8). Of
were females and 9(25.0%) were
the nine with HIV- TB coinfec-
males. Thirty
(83.3%) were of
tion, the clinical presentation were;
lower socioeconomic class. His-
PTB 5(55.6%), and
tory of contact with a case of TB
extrapulmonary 4(44.4%).
was obtained in 17(47.2%). The
Conclusion: The
patterns of
TB in
commonest symptoms identified
adolescents are admixture as seen
in
these adolescents were; cough
in
younger children and adult from
27(75.0%),
weight
loss
22
clinical and radiological character-
(61.1%), fever18(50.0%), sputum
istic findings. TB remains a pre-
14(38.9%), body swelling
ventable disease condition and is
7(19.4%), hemoptysis 2(5.6%);
curable
with early appropriate
while signs were underweight,
treatment
pyrexia and chest findings. Nine
(25.0%) had associated retroviral
Key words :
Adolescent tuberculo-
disease. Thirty four (94.4%) pre-
sis, clinical pattern.
sented at time of diagnosis with
Introduction
bers of the general population
2,3 . In 2012, WHO esti-
mates that 8.6 million incident cases of TB were re-
The adolescent person whose age is between 10 -19
ported with 530,000 new case of TB being children less
than 15 years and 74,000 child deaths from the disease .
2
years, has been described generally to be a healthy
group compared to the general population, despite their
These estimate were higher than the report published in
known high risk behavior . The adolescent who is also a
1
the preceding year reflecting that more TB cases were
being notified among children globally . Over 30
2
young person suffers from TB along with other mem-

332
million Nigerians (approximately 22 percent) are be-
The protocol for diagnosis of tuberculosis in the clinic
tween the ages of 10-19. The adolescents and Young
4
were based on:
people represent a high risk sexual behavior groups that
are
highly vulnerable to HIV /AIDs infection and conse-
Bacteriological identification of mycobacterium tuber-
quently at risk of TB, in the dual pandemic .
5
culosis complex by direct smear microscopy performed
using auramine-rhodamine and confirmed with Kinyoun
The
younger child, under five have been shown to be at
stain on clinical specimen in a patient with suggestive
greater risk of TB especially in the presence of malnutri-
symptoms and signs or
tion
and lower family socioeconomic background .
6,7
Clinical diagnoses based on a combinationof symptoms
Childhood TB cases proportions in countries vary from
and
signs in the presence of any one or more of the fol-
3-
40percent . Nigeria is among the 22 high burden
2
lowing; a tuberculin skin test (TST) ≥ 10 mm for patients
nations with TB, accounting for 80percent of the world
that are HIV negative or >5 mm in HIV positive pa-
TB
cases. An estimated 1.1 million (13percent) of the
tients, a history of contact with suspected tuberculosis
8.6 million people who developed TB in 2012 were HIV
patient, radiological and/ or histo-pathological finding
positive with 75 percent in the African region . This
2
from lymph node biopsy suggestive of TB. Such clini-
ancient and still ongoing TB scourge is caused by the
cal features include a history of cough lasting for two
mycobacterium tuberculosis complex, with
high and
weeks or more, sputum with or with haemoptysis, pro-
low prevalence worldwide despite available measures
longed fever for which patient has been treated with
that highlight how to addressed and control the disease.
8
antibiotics with no improvement, weight loss or malnu-
9
The young person will be at risk of TB infection when
trition and poor appetite. Other symptoms include con-
in
contact with a case of TB disease who is actively
vulsions, loss of consciousness, swelling in the back or
coughing, especially when he is immune compromised,
any other part of the body. Signs recorded were also
is
homeless or lives in congested camps, prison or jail,
retrieved including laboratory test results, treatment
or
nursing home and have risky behaviors such as intra-
given with duration and outcome. Cultures were not
venous drug use
2,
3
.
done on any of the specimens. Only children aged less
than 16 years were seen at the paediatric respiratory
There are few reports that have focused on TB burden in
clinic as part of the hospital policy, while those 16 years
the adolescent. In the United States, adolescents com-
and above were attended to by the adult physicians.
prised approximately one-third of the pediatric cases
reported from 1994 to 2010 . The younger child, par-
3
A
proforma was used to extract information relating to
ticularly the under-fives play little role in the transmis-
patient demography, clinical symptoms and signs, his-
sion of TB because they more often have negative
tory of contact, pattern of TB, radiological features,
smears; they rarely have cavitary disease; they often
treatment and outcome (completion of treatment, lost to
have little or no cough; and when cough is present, it is
follow up or retreatment for TB). All the patients were
generally not forceful enough to expel aerosolized ba-
under care by the authors and case folders retrieved were
cilli efficiently.
10
In
contrast, the 10- to 19-year age
analyzed after approval was obtained from the institu-
group presents a different spectrum of disease manifes-
tional review board of the National hospital Abuja. Data
tations, including adult-type disease, from which respi-
were analyzed using Microsoft excel 2010 and mean
ratory samples can be more readily obtained . The Stop
2
(SD), percentages and tables were generated.
TB
Partnership goals include reducing the global burden
of
TB (prevalence and mortality) by 50 per cent in 2015
compared with 1990 levels and eliminating TB as a pub-
lic health problem by 2050 . In other to achieve this
11
Results
goal, the adolescent though largely a subset of the paedi-
atric age group but differ remarkably from the younger
A
total of 52 adolescents aged 0-15 years diagnosed
child should be viewed differently since preventive
with tuberculosis were documented in the paediatrics
measure for TB differ for the child and the adult.
respiratory clinic record, but only 36 case folders with
The study aims to describe the clinical presentation and
adequate information retrieved from the hospital medi-
outcome of adolescent tuberculosis at National Hospital
cal records were analyzed during the period August
Abuja (NHA), Nigeria.
2009 to July 2013. This gives a prevalence rate of 18.8%
(36/192). The mean (SD) age was 12.3(1.76). 75.0% of
the adolescents were females while 83.3% were of lower
socioeconomic group as shown in table 1.
Subjects and Method
Table 1: Socio-demographic
characteristic of
the study
popu-
This
is a retrospective, descriptive study, conducted at
lation
Variable
N
%
the Paediatric Respiratory Clinic of National Hospital
Abuja. The clinic is held once weekly with average
Sex
Male
9
25.0
attendance of 15 patients seen per week. The case fold-
Female
27
75.0
ers of adolescents aged 10- 15 years seen at the clinic
Socioeconomic status
from August 2009 to July 2013 who were diagnosed
High social class
6
16.7
with tuberculosis were retrieved.
Lower social class
30
83.3
333
34
patients (94.4%) were diagnosed after they presented
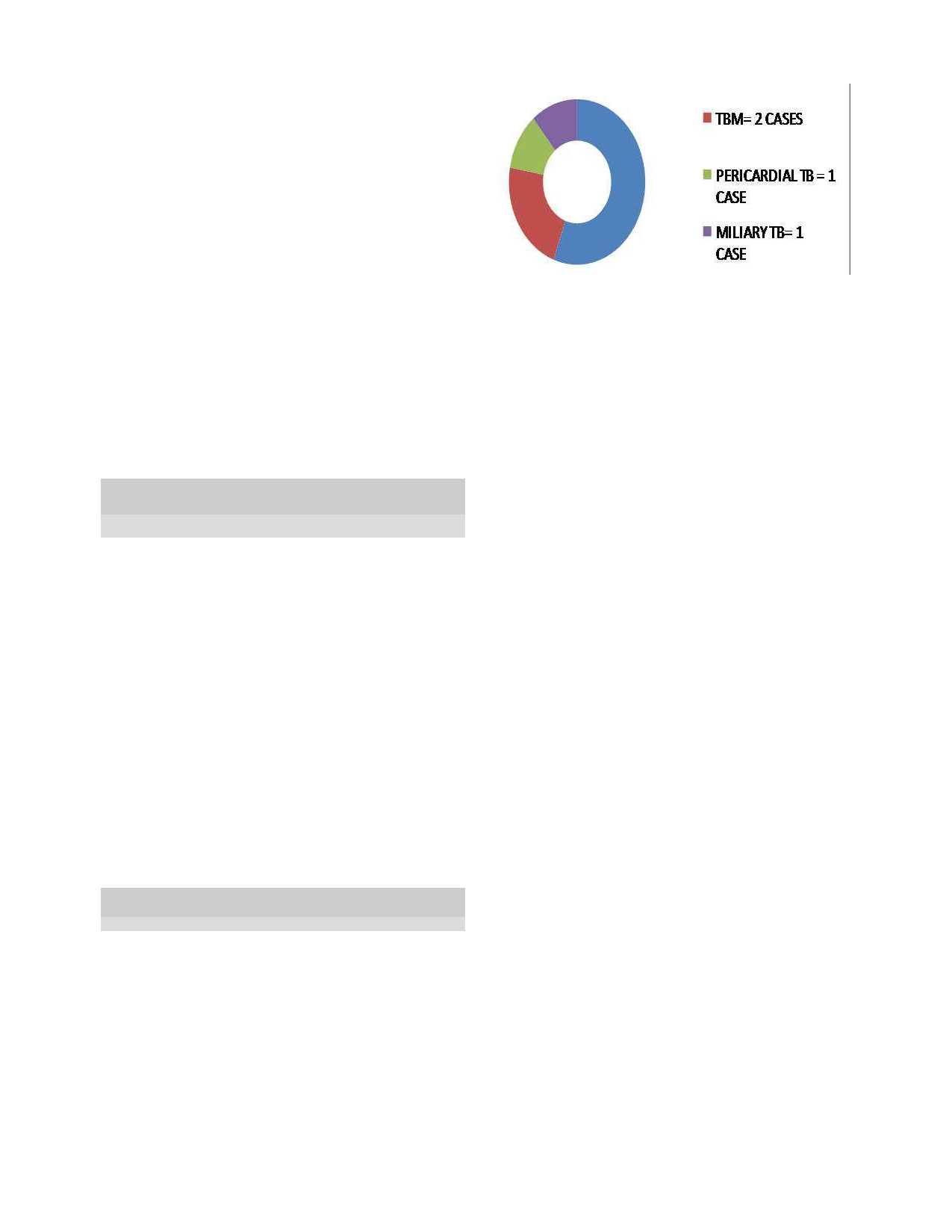
Chart 1: TB
pattern in
adolescent with
retroviral disease
with clinical symptoms while 2(5.6%) were identified
through contact tracing as asymptomatic (latent TB
cases). 17(47.2%) adolescents had a history of contact
with a person with suspected TB while 9(25.0%) had
associated retroviral disease. Thirty two (88.9%) had a
history of BCG given within one month of life. The
most common symptoms identified were cough, weight
loss and fever, while major signs were underweight,
pyrexia
and
chest
findings
(respiratory
distress,
tachpnoea, crepitations, decreased percussion note and
chest expansion); table 2.
Acid- alcohol fast bacillus (AFB) was isolated in 5
(13.9%) and 23 (63.9%) had a raised ESR above 30mm/
hr, Abnormal chest radiograph findings were; wide-
spread lung infiltrate 10 (27.8%), hilar opacities
Discussion
7(19.4%), cavitory lesions 4(11.1%), pleural effusion
3(8.3%) and miliary opacities 1(2.8%). Twenty seven
The study describes the clinical characteristics of adoles-
(75.0%) of the adolescents completed treatment for
cent TB at the National Hospital Abuja. Adolescent TB
tuberculosis, 7(19.4%) were lost to follow up and
accounted for 18.8 percent of cases of TB seen during
2(5.6%) died., while 4(11.1%) had re-treatment for TB
the study period. The female was at greater risk of TB in
due to relapse.
this report. Studies have documented that the prevalence
of
TB in children is higher in girl until between the age
10
and 16 years . The gender disparity becomes evi-
12
Table 2: Common
symptoms and
signs identified
in adoles-
cent TB
dence after fifteen years with a rising rate amongst male
up
till adulthood . Majority of the cases had active dis-
12
Symptoms
N
%
ease. This may be the reason why the prevalence was
Cough
27
75.0
Weight loss
22
61.1
higher in the female since the progression from infection
Fever
18
50.0
to
active disease is more rapid in the female gender early
in
life and the reverse at older age
12,13
Sputum
14
38.9
.
The young girl
Body Swelling (various sites)
7
19.4
has
been shown to have a threefold higher to acquire
Headache
3
8.3
HIV infection when compared to the male of same
Hemoptysis
2
5.6
age. This risk factor for HIV may also contribute to
Swelling in the back
1
2.8
early active disease progression . Other factors that
10
Signs
have been known to account for considerable variability
Underweight ≤ 80%
24
66.7
in
the outcome of M. tuberculosis infection include mal-
Pyrexia
17
47.2
Pallor
16
44.4
nutrition, poor socioeconomic status and immune sup-
pression such as caused by HIV
4,5,14-16
Chest findings
15
41.7
.
Over 60 percent
Hepatomegaly
11
30.6
of
the study populations were undernourished with
Lymphadenopathy
7
19.4
weights 80 percent or less for age and sex. Malnutrition
Gibbus (thoracolumbar)
2
5.6
interferes with the cell mediated immunity (CMI) re-
Neck stiffness
1
2.8
sponse and therefore contributes to much of the in-
creased frequency of TB in impoverished patients .
16
The clinical presentations of TB were; %) pulmonary
TB
(PTB) 22(61.1) and
extra-pulmonary TB 14
The TB rates were highest in the adolescent of lower
(38.9%); table 3
socioeconomic status. The historical association of TB
with low socioeconomic status and poverty had long
been established
14,15
Table 3: Clinical
presentation of
TB in
the adolescents
.
HIV/AIDS–TB co- infection co-
Variable
N
%
existed in twenty five percent of the adolescents. The
dual disease burdens are known to adversely affect the
Latent TB
2
5.6
outcome of each other. HIV impairs the host cellular
Pulmonary TB
22
61.1
Smear positive
5
13.9
immunity to contain TB infection and verse visa. The
Smear negative
17
47.2
combination with HIV co-infection, dramatically com-
Extrapulmonary TB
12
38.9
promises host resistance to TB, leading to high disease
TB
adenitis
4
11.1
prevalence in affected endemic populations that include
TB
meningitis
3
8.3
the adolescent. With the current over half a million ado-
TB
pericarditis
3
8.3
lescent infected with TB as at 2012, the risk for in-
2
Tb
spinal
1
2.8
creasing prevalence of multidrug-resistant (MDR) and
Milary TB
1
2.8
extensively drug-resistant (XDR) MTB strains and the
17
Of
the nine cases with HIV-TB co- infection, 5(55.6%)
more recent occurrence of TDR (totally drug-resistant)
MTB strains, which are virtually untreatable
18
presented pulmonary disease while remaining 4 had
becomes
extra- pulmonary diseases; namely TBM 2; pericardial
a
challenge to all for early detection and treatment of all
TB
and miliary TB one each; in Chart 1
cases of TB.
334
Evidence of late presentation in 94.4 percent of the ado-
the
first years of life, however doesn’t prevent pulmo-
lescents
studied was the presence of clinical symptoms
nary
TB, which is prevalent in the adolescents and
at
time of diagnosis. Such adolescents’ patients would
adults, who mostly spread the infection. A BCG that
have
already contributed to infection transmission espe-
will
prevent progression of latent TB to active disease
cially as they cough with sputum production in the pres-
would be desirable; hence a vaccine that is more effec-
ence
of AFP positive status acting as reservoir of infec-
tive
and safe against TB remains a task. The possible
tion
to contacts. Late diagnosis results from this lack of
role
of a booster or replacement in the ongoing BCG
early clinical suspicion of the disease. Cough was the
trials may in future provide the solution to TB infection
in
the population that includes adolescents .
25
commonest
symptom
in
the
adolescent
while
38.9perecnt were able to produce sputum, unlike the
younger child who most times cannot expectorate volun-
The patterns of TB in adolescents seen are a mixture of
tarily. Cough as a significant symptom was also found
childhood forms and adult patterns in their clinical, ra-
to
be specific in a report by Marais et al
19
in
which a
diological and microbiological findings. Most of the
persistent, non-remitting cough was reported in 15/16
childhood TB forms seen were smear negative PTB
similar to the finding reported by Cruz AT et al.
3
(93.8%) children under 13years with tuberculosis and in
For
2/135 (1.5%) children and young adolescents, without
the extra- pulmonary forms, hilar lymphadenopathy was
tuberculosis, indicating a specificity of 98.5%(135/137)
commonest followed by tuberculous meningitis and
19
.
The use of well-defined symptoms, even in re-
pericarditis occurring in equal proportion. A similar pat-
source limited settings offer some value in the diagno-
tern was also identified in the adolescent with retroviral
sis of childhood and adolescent pulmonary tuberculosis.
disease.
Sputum production with acid-alcohol fast bacillus
(AFB) smear positivity is risk factors for transmission of
Imaging studies such as chest radiograph plays a signifi-
infection among the adolescents and among his peers
cant role in childhood TB diagnosis. A normal radio-
graphic study does not however rule out TB . Abnormal
26
due
to the high social interaction associated with this
age
group. Close to 14 percent were bacteriological con-
chest radiograph findings were mostly widespread lung
firmed cases of TB in the present report. Contact with
infiltrate (27.8 percent), hilar opacities (19.4percent),
person with suspected TB is an important factor for ac-
cavitatory
lesions
(11.1percent),
pleural
effusion
quiring the infection seen in up to 47.2 percent of the
(8.3percent) and miliary opacities (2.7percent). Tradi-
adolescents. Early case finding from screening of con-
tionally, the two radiological patterns of TB manifesta-
tacts of adolescents and adult cases of active cases re-
tions that have been described are the primary TB and
mains a strategy for the prevention and control of TB.
reactivation (post-primary) TB which relate to the pa-
tient immunity . The present study shows a mixed form
27
This also includes the use of isonaizid prophylaxis espe-
cially in under five children exposed to contacts of ac-
of
both primary disease and reactivation TB, though
tive disease and HIV positive persons. All adolescents
primary pattern was more predominant. Children and the
with a contact history must be evaluated with a TST for
immunocompromised persons usually present with fea-
LTBI. Two cases were found to have LTBI in this re-
tures of primary TB which includes; parenchymal infil-
view and treated. The practice of LTBI treatment for TB
trates or consolidation within the lung parenchyma, in-
contacts with a TST size of 10mm and above help re-
volving any pulmonary lobe or segment, hilar lymph
duce progression to disease. This routine use of isoni-
node with or without atelectasis and unilateral pleural
azid preventive therapy (IPT) is an effective and cost-
effusion on the same side of the primary focus of the
TB
. In Reactivation TB, apical consolidations involv-
28
effective intervention among child household contacts.
ing the upper lobe or superior segment of lower lobe are
The use of Bacillus Chalmette –Guerin (BCG) vaccine
commonly seen with other features of cavitation, soli-
tary nodules and military picture min some cases . The
28
was
high among the adolescents.
The BCG vaccine
have been shown to have from zero to 80 percent effec-
primary forms of TB were mostly those of hilar lymph
node enlargement, (52.8 percent). Marias et al reported
29
tiveness in preventing tuberculosis for a duration of 15
years; however, its protective effect appears to vary ac-
that up to 90- 95 percent of primary Tb in children are
cording to geography and the laboratory in which the
hilar lymph node enlargement which could be unilateral
vaccine strain was grown
20,21
.
A 1994 systematic review
or
bilateral and widespread in up to70 percent.
found that the BCG reduces the risk of getting TB by
about 50%; (relative risk (RR) of TB of 0.49 (95% con-
Completion of treatment in TB is a significant part of
fidence interval [CI], 0.34 to 0.70) for vaccine recipients
disease control, as this stops transmission of infection
compared with non-recipients (protective effect of 51%),
from
an active case to contacts. A 75percent complete
and
a protective effect from tuberculous deaths of 71%
treatment rate in the present report was slightly lower
(RR, 0.29; 95% CI, 0.16 to 0.53), and a protective ef-
than the reported 85percent national figure (Nigeria
2009 –2013) . A loss to follow up or default from treat-
30
fect for meningitis of 64% (OR, 0.36; 95% CI, 0.18 to
0.70) .
22
BCG is effective against rare forms of severe
ment and poor compliance are risk factors for continuing
childhood TB meningitis and miliary disease, however,
infection transmission in the community with risk for
the variation in protection against common pulmonary
resistance development and drug resistance TB. Lost to
TB
that BCG offers has generally been disappointing in
follow up rate was 19.4percent; which is lower than ear-
trials conducted in the developing world
23,24
.
This pro-
lier report by Jiya et al (36.5%) from Sokoto in north-
west of Nigeria . The Directly Observed Therapy (DOT)
5
tection of BCG for children from severe forms of TB in
335
strategy aim to improve treatment compliance and com-
Conclusion
pletion for the patients through a reliable supervisor of
patients and accurate record keeping. TB treatment in
Tuberculosis remains a significant public health prob-
the adolescent can be a challenge resulting from the di-
lem, particularly in resource limited settings like
verse behavioral, social and economic demography asso-
Nigeria. Late presentation was high in majority of ado-
ciated with the development of the adolescent. This can
lescent as they were symptomatic already before presen-
lead to treatment discontinuation, resulting in perpetua-
tation for diagnosis. A mixed pattern of disease was seen
tion of TB transmission in the community and appear-
in
the adolescent for a disease condition that remains
ance of resistant strains. Death rate among the adoles-
preventable and treatable.
cent was 5.6 percent; similar to the overall TB deaths of
five percent for 2010 (Nigeria) .
31
References
1.
World Health Organization, online
11.
World Health Organization 2011.
20.
Sterne J. A., Rodrigues L. C.,
article; Adolescent health. Link:
The
global plan to stop TB 2011–
Guedes
I. N. Does the efficacy of
http://www. who.int/topics/
2015.
http://www.stoptb.org/
BCG
decline with time since vac-
adolescent_health/en/ (Accessed:
assets/documents/global/plan/
cination? Int.
J. Tuberc.
Lung Dis .
26/10/2013)
TB_GlobalPlanToStopTB2011-
1998; (2) 200–207.
2.
World Health Organization, Ge-
2015.pdf.
21.
Ottenhoff TH, Kaufmann SH. Vac-
neva. Global Tuberculosis Report
12.
World Health Organanization.
cines against tuberculosis: where
2013.Link:http://apps.who.int/iris/
Online article: Gender and Tuber-
are
we and where do we need to
bitstream/10665/91355/1/
culosis. Link: whqlibdoc.who.int/
go? PLoSPathog .
2012; 8(5),
9789241564656_eng.pdf?ua=1
gender/2002/a85584.pdf (Accessed
1002607
(Accessed 26/10/2013)
12/12/2013)
22.
Colditz GA, Brewer TF, Berkey
3.
Cruz AT, Hwang KM, Birnbaum
13.
Hudelson P. Gender differentials
CS,
Wilson ME, Burdick E, Fine-
GD,
Starke JR. Adolescents with
in
tuberculosis: the role of socio-
berg HV, Mosteller F. Efficacy of
Tuberculosis. A Review of 145
economic and cultural factors.
BCG
vaccine in the prevention of
Cases. Pediatr
Infect Dis
J .
Tubercle and Lung Disease
tuberculosis. Meta-analysis of the
2013;32(9):937-941
1996;77:391e400.
published literature. JAMA 1994
;
4.
Esiet AO. Action Health Inc. Ado-
14.
Gustafson P, Lisse I, Gomes V,
271(9):698-702
lescent Sexual and Reproductive
Vieira CS, Lienhardt C, Naucler A,
23.
Fifteen year follow up of trial of
H
eal th
in
Ni
geri a.
Wh
y
Jensen H, Aaby P. Risk factors for
BCG
vaccines in south India for
“Adolescent
Sexual and Repro-
positive
tuberculin skin test in
tuberculosis prevention. Tubercu-
ductive Health”. Link: http://
Guinea-Bissau. Epidemiology .
losis Research Centre (ICMR),
www.wilsoncenter.org/sites/
2007; 18:340–7.
Chennai. Indian
J. Med.
Res . 1999;
d e
f a u l t / f i l e s / E s i e t %
15.
Grigg ER. The arcana of tubercu-
110: 56–69
20Presentation.pdf (Accessed
losis with a brief epidemiologic
24.
Rodrigues L. C., Diwan V. K.,
20/11/2013)
history of the disease in the USA.
Wheeler J. G. Protective effect of
5.
World Health Organanization.
Am Rev Tuberc. 1958;78:151–72.
BCG
against tuberculous meningi-
online article: Nigeria- link:
16.
Cegielski JP, McMurray DN.The
tis
and miliary tuberculosis: a meta
www.who.int/countries/nga/en/
relationship between malnutrition
-analysis. Int.
J. Epidemiol .
1993;
(Accessed: 27/11/2013)
and
tuberculosis: evidence from
22:1154–1158
6.
Ibadin MO, Oviawe O. Trends in
studies in humans and experimen-
25.
McShane H. Tuberculosis vac-
childhood tuberculosis in Benin
tal
animals. Int
J Tuberc
Lung Dis.
cines: Beyond BacilleCalmette–
City,
Nigeria .
Ann Trop
Paed
2004 (3):286-98.
Guérin. Philos
Trans R
SocLond B
2001; 21:141-145
17.
Gandhi NR, Nunn P, Dheda K,
Biol Sci. 2011; 366(1579): 2782–
7.
Jiya NM, Bolajoko TA, Airede KI.
Schaaf HS, Zignol M, et al. Mul-
2789.
Pattern Of Childhood Tuberculosis
tidrug-resistant and extensively
26.
Lamont AC, Cremin BJ, Pelteret
In
Sokoto, Northwestern Nigeria.
drug-resistant tuberculosis: a threat
RM.
Radiological pattern of Pul-
Sahel Medical Journal
2008;11
to
global control of tuberculosis.
monary tuberculosis in the paediat-
(4):110-113
Lancet 2010; 375: 1830–1843.
ric
age group .
Pediatr Radiol
8.
Wu
XR, Yin QQ, Jiao AX, Xu
18.
Velayati AA, Masjedi MR, Farnia
1986; 16: 2-7.
PB,
Sun L, Jiao WW, et al.
P,
Tabarsi P, Ghanavi J, et al.
27.
Awil PO, Bowlin SJ, Daniel TM.
“Pediatric
Tuberculosis at Beijing
Emergence of new forms of totally
Radiology of pulmonary tuberculo-
Children’s Hospital: 2002-2010
,”
drug-resistant
tuberculosis bacilli:
sis
and HIV infection in Gulu,
Paediatrics , 2012; 130(6):1433-
super extensively drug-resistant
Uganda .
EurRespr J .
1997; 10:
615
1440.
tuberculosis or totally drug-
-618
9.
Winston C, Menzies H. Pediatric
resistant strains in iran .
Chest
28.
Ogbeide O. The radiological man-
and
adolescent tuberculosis in the
2009; 136: 420–425.
agement of tuberculosis. Benin
United States, 2008-2010.
Pediat-
19. Marais
B, Gie
R, Obihara
C, Hes-
journal of postgraduate medicine
.
rics . 2012;130(6) 1425-
1432
seling A, Schaaf H, and Beyers N.
December 2009; 11: 74 – 78.
10.
Lawrence RM. Tuberculosis in
Well defined symptoms are of
children. In: Rom WN, Garay SM,
value in the diagnosis of childhood
eds. Tuberculosis. Boston: Little,
pulmonary tuberculosis .
Arch Dis
Brown, 1996:675-88.
Child. 2005; 90(11): 1162–1165.
336
29.
Marais BJ, Gie RP, Schaaf HS,
30.
World health Organization online
31.
Nigeria Tuberculosis Fact Sheet.
Hesseling AC, Enarson DA, Bey-
article. Global Health Observatory
United States Embassy in Nigeria.
ers
N. The spectrum of childhood
(GHO).How many TB cases have
Link:http://photos.state.gov/
tuberculosis in a highly endemic
been
successfully
treated?
libraries/nigeria/487468/pdfs/
area . Int
J Tuberc
Lung Dis
2006;
Link:http://www.who.int/gho/tb/
JanuaryTuberculosisFactSheet.pdf.
10:732-738.
epidemic/treatment/en/. (Accessed
2012. (Accessed 10/1/2014).
10/1/2014).